Introduction
Arthritis is inflammation of a joint. It can lead to pain and swelling of the joint. Ankle arthritis is inflammation of the ankle joint. It is nine times less common than arthritis of the knee and hip joint. Causes of ankle arthritis include:
- Primary osteoarthritis
- Post-traumatic
- Rheumatoid arthritis
- Osteonecrosis
- Neuropathic
- Septic
- Gout
- Haemophiliac
Among these causes, post-traumatic is the most common cause and it accounts for over 60% of all ankle arthritis.
Symptoms
Patients may complain of pain on weight bearing or during motion. The pain may exacerbate after vigorous activities. There could also be joint swelling, redness, warmth and loss of ankle motion. Patients may find difficulty in walking and may require the use of walking aids.
Signs
There could be ankle deformity and tenderness along the ankle joint line. The joint might also be warm and swollen. The passive and active range of movement of the ankle might be reduced. In early stage of arthritis, ligament laxity would also be tested especially in patients with history of recurrent sprain. In the late stage of arthritis, stiffness is more frequently presented and may mask the underlying ankle ligament laxity.
Investigations
After history and physical examination, blood tests may be required to test for inflammatory markers to rule out rheumatoid arthritis, gout and other auto-immune diseases. Standing X-ray of the foot and ankle would be taken. Sometimes, computerized tomography or magnetic resonance imaging might also be performed to assess the underlying cause of ankle arthritis.
Classification
Takakura Classification is frequently used to classify ankle arthritis radiologically. It may implicate the subsequent options of treatment according to the staging. Stage I is early sclerosis and osteophytes formation. Stage II is narrowing of joint space without bone contact. Stage III with narrowing of joint space with bone contact. Stage IV is complete bone contact. In some patients, Computerized Tomography (CT) and Magnetic Resonance Imaging (MRI) might be useful to determine the severity of the disease. [Figure 1]

Treatment
Conservative Treatment
Treatments depend on symptoms and staging of the disease. For early arthritis, conservative treatments should be considered first.
1. Anti-inflammatory medications – Medications including non-steroidal anti-inflammatory drugs (NSAIDs), topical ointments and patches can be used.
2. Life style modifications – Some activities should be modified so as to slow down the progression of the arthritis. Patients are advised to minimize activities which aggravate the ankle pain and change high-impact sports including tennis and badminton to swimming or jogging, etc. Patients are also advised to lose weight in order to reduce stress on the ankle joint.
3. Physical therapy – A physical therapist will help with specific exercises which help decrease ankle swelling, improve the range of movement as well as flexibility of ankle.
4. Orthosis – Bracing is sometimes needed to unload and reduce irritation to the ankle joint. An ankle-foot orthosis helps mobility and reduce pain. Custom-made insoles are also used to minimize pressure on the foot and ankle.
5. Injections – Steroid injections may provide short-term relief of pain. Intra-articular hyaluronic acid injection can be considered but its role is still controversial. Recently, more studies have shown that platelet-rich plasma injection is a valid and safe alternative to postpone the need for surgery.
Surgical Treatment
It is recommended when conservative treatments fail.
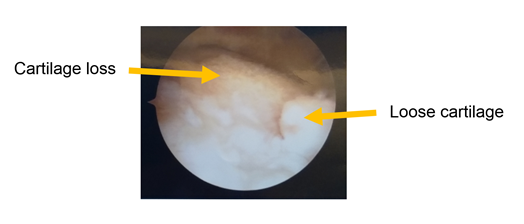
1. Arthroscopic debridement – It is recommended in patients with early ankle arthritis. Debridement is done to remove inflamed synovium, loose cartilage fragments, osteophytes and loose bodies in the ankle joint which might affect the range of movement. In arthroscopic surgery, a small camera is placed into the joint for reviewing through a stab incision; and another incision is made for placing instruments into the joint to retrieve the debrided substances. Arthroscopic debridement is most successful in patients with early ankle arthritis where the arthritis does not cause any decrease in joint space yet. [Figure 2]
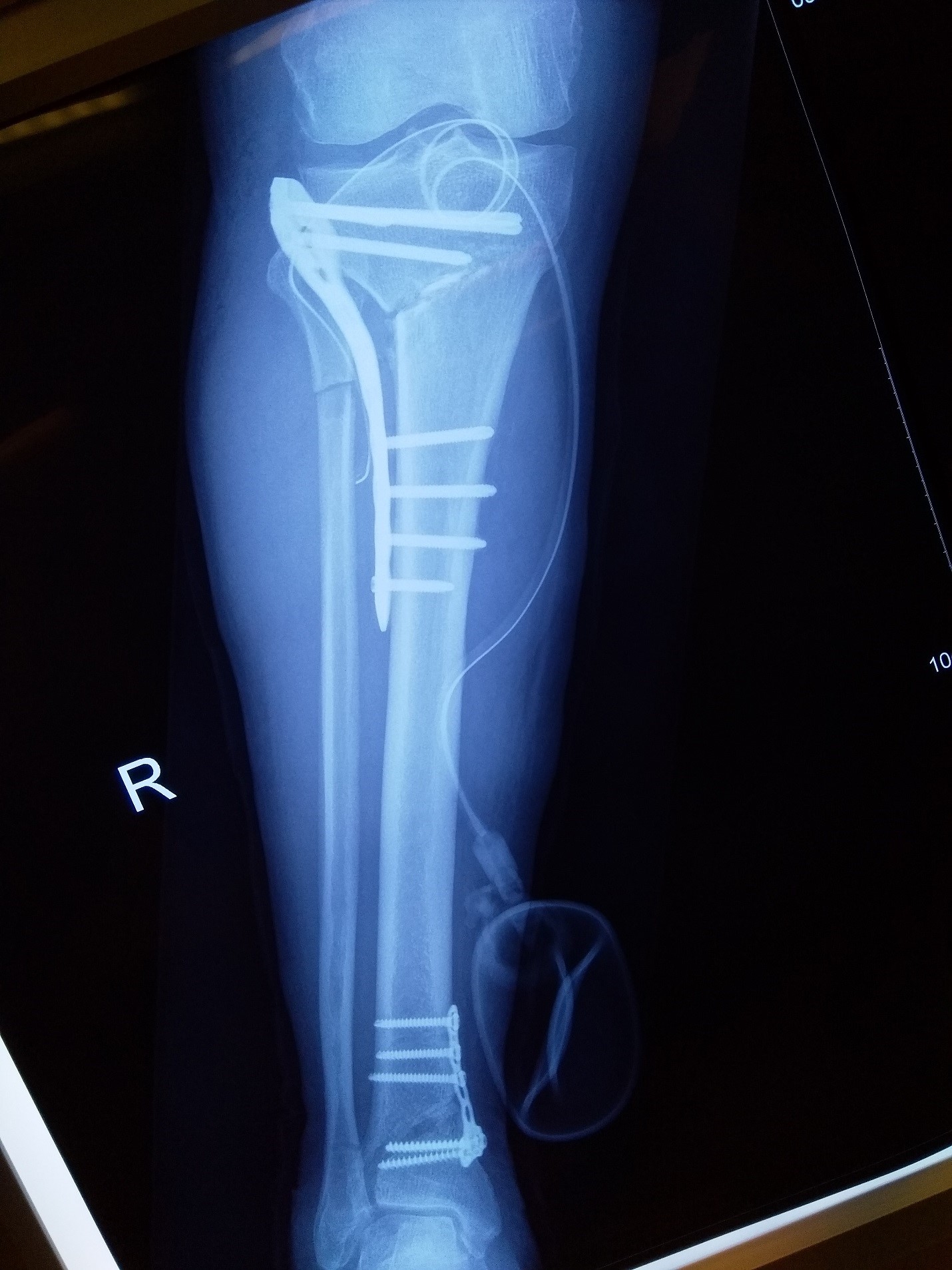
2. Osteotomy – For patients with more advanced ankle arthritis, there might be narrowing of joint space and altered lower limb alignment, osteotomy can be considered. Osteotomy means cutting of bone to correct the alignment. [Figure 3]
3. Distraction arthroplasty – It is another option for younger patients but there is still not much evidence to support its role.
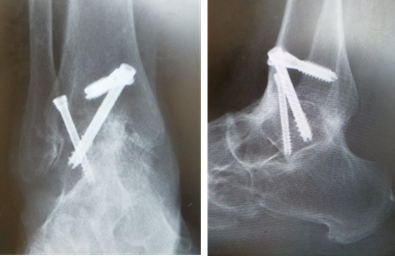
4. Ankle fusion – It remains an option to treat end-stage ankle arthritis and results in significant improvement in terms of pain and function. It is considered as the gold standard for the treatment of end-stage ankle arthritis. It could be done with arthroscopic assistance or in open surgery. [Figure 4]
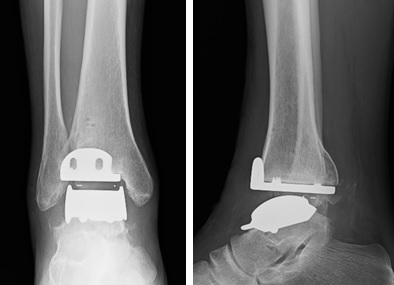
5. Total ankle replacement – It has the advantages of preserved movement and less stress on the neighboring joints. Second generation implants have been shown to have encouraging intermediate clinical results. Its long term result has been improved and comparable to the gold standard. [Figure 5]
References
- Thomas RH, TR Daniels. Ankle arthritis. J Bone Joint Surg Am. 2003 May; 85-A [5]:923-36.
- Saltzman CL, Salamon ML, Blanchard GM, Huff T, Hayes A, Buckwalter J, et al. Epidemiology of ankle arthritis: report of a consecutive series of 639 patients from a tertiary orthopaedic center Iowa. Orthop J.2005; 25:44-6.
- Emmanouil D. Stamatis, M.D., Paul S. cooper, M.D., Mark S. Myerson, M.D. Supramalleolar osteotomy for the treatment of distal tibial angular deformities and arthritis of the ankle joint. Foot Ankle Int. 2003 Oct; 24(10):754-64.
- Ankle arthritis and the treatment with ankle replacement. Rev.Med.Clin.Condes. 2014; 25(5):812-823.
- Repetto I, Biti B, Cerruti P et al. Conservative Treatment of Ankle Osteoarthritis: Can Platelet-Rich Plasma Effectively Postpone Surgery? J Foot Ankle Surg. 2017 Mar-Apr; 56(2):362-365.
Written by Dr. Diane Tai Hei-yan
20 January 2021